DALK: Deep Anterior Lamellar Keratoplasty
DALK (Deep Anterior Lamellar Keratoplasty) is a partial-thickness corneal transplant. It involves replacing the damaged outer and middle layers (the stroma) while preserving the patient’s own innermost layer (the endothelium), provided it is still functioning correctly.
This technique is particularly effective for treating certain corneal conditions, such as keratoconus, as it significantly reduces the risk of graft rejection compared to a full-thickness transplant.


How does it work?
Learn more about the procedure / equipment

Removal of the anterior layers (epithelium and stroma) down to Descemet's membrane. The endothelium is preserved intact, ready to receive an endothelium-free graft.
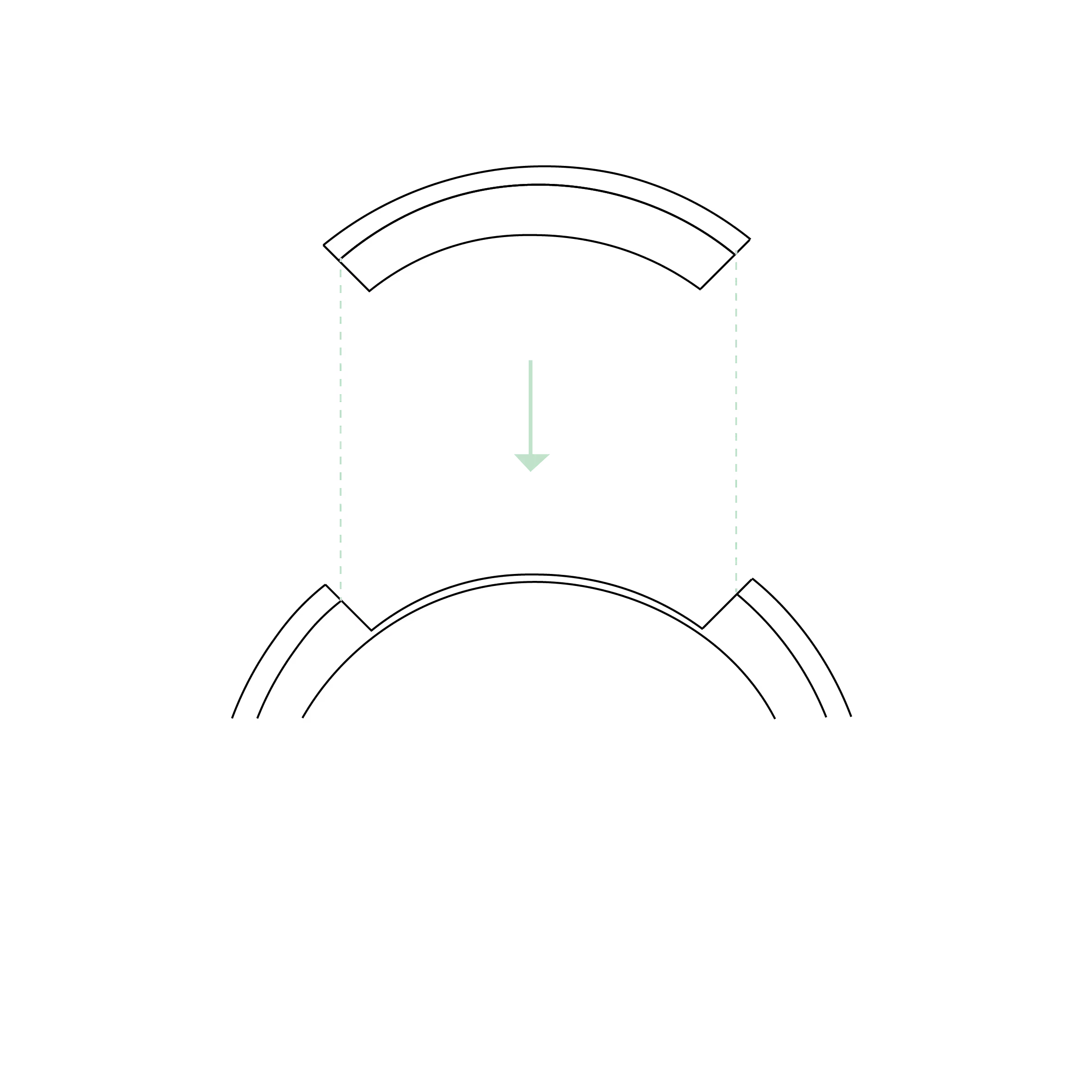
Placement of the donor corneal graft, consisting of the anterior layers (epithelium and stroma), onto the patient's intact Descemet's membrane.
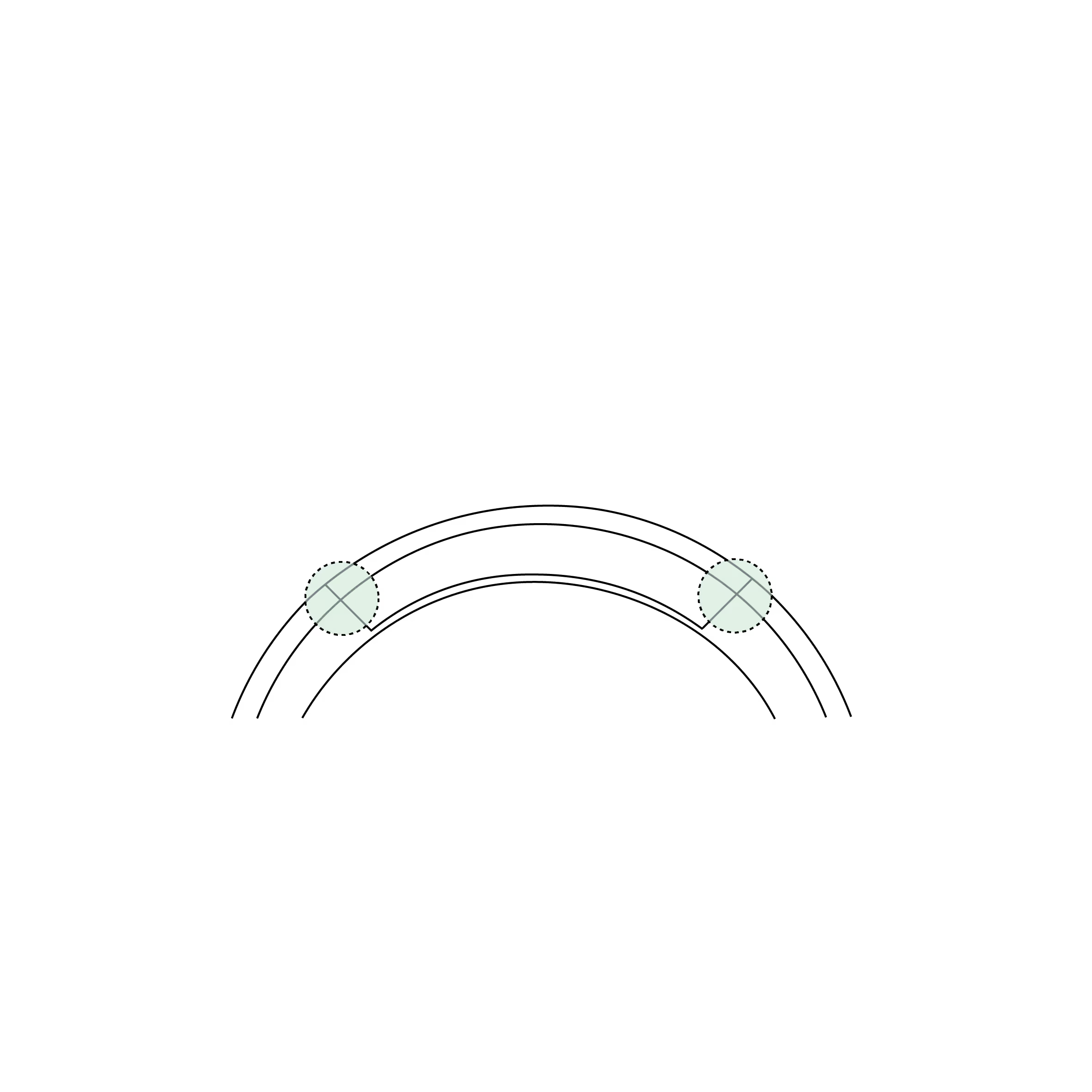
The graft is secured with fine sutures (10 times finer than a human hair). These are placed evenly, ensuring the stability and alignment of the graft on the patient's cornea.
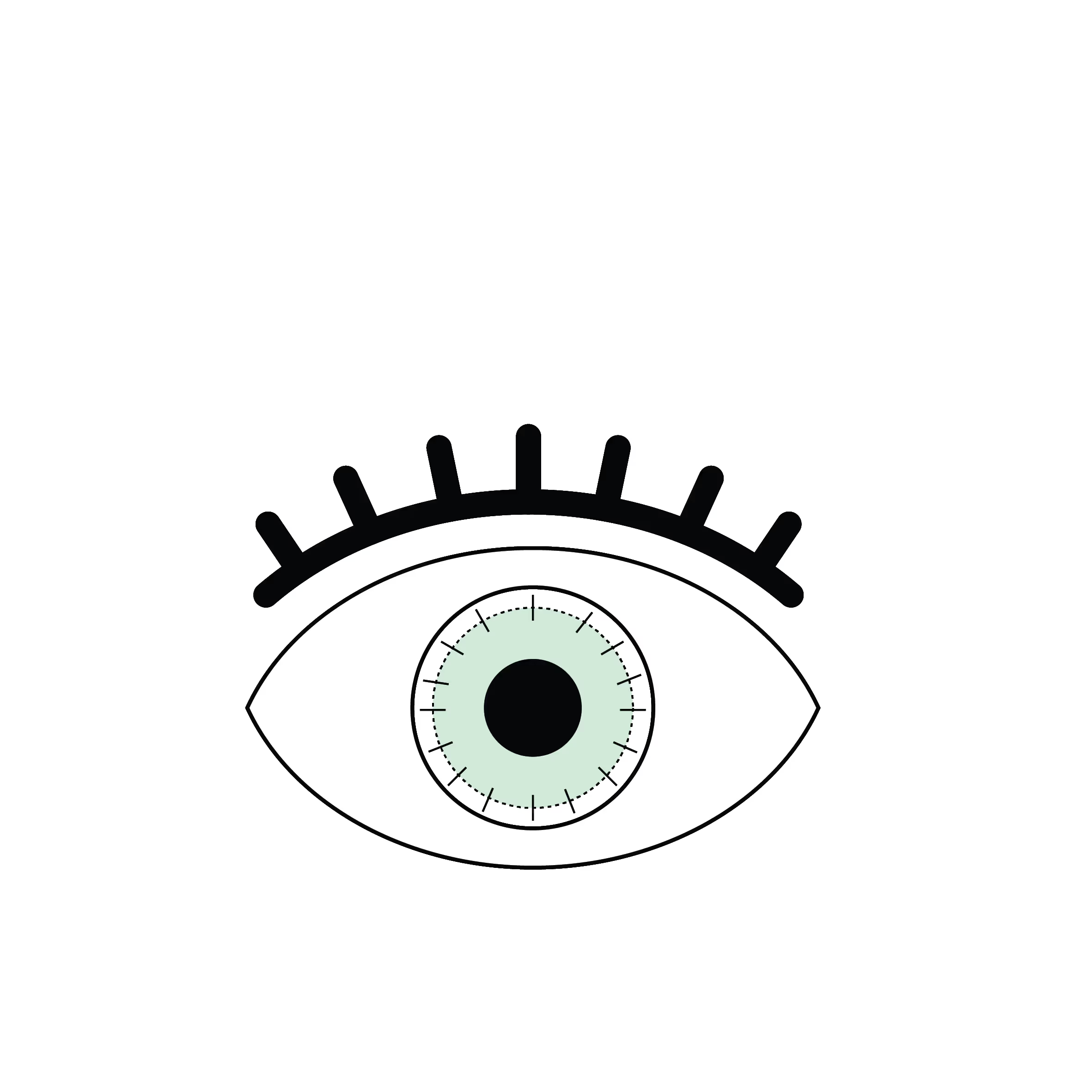
Circular graft held in place by fine sutures.
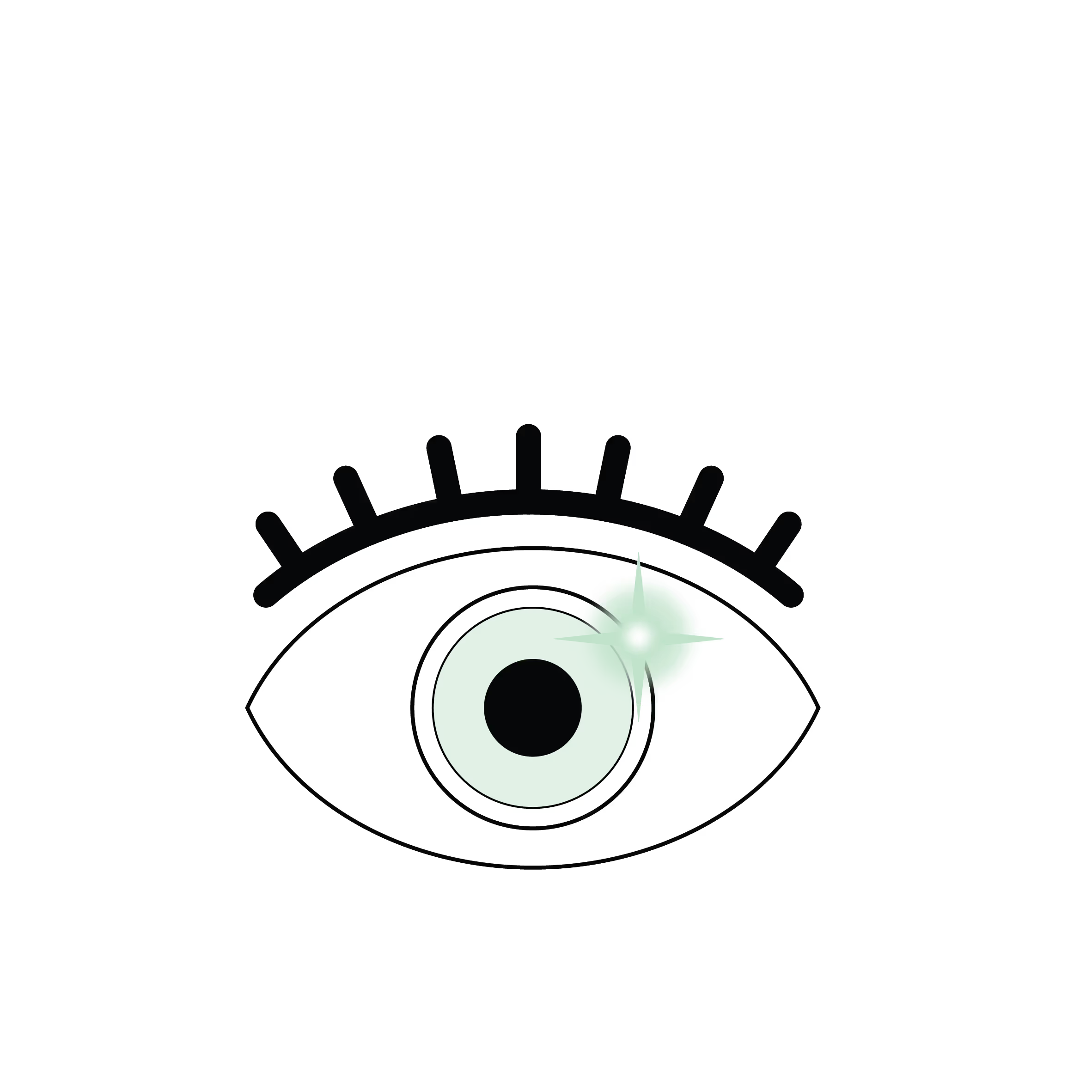
Cornea after suture removal. The graft is barely visible, perfectly integrated, with restored corneal transparency and vision.
What is DALK?
DALK (Deep Anterior Lamellar Keratoplasty) is a surgical technique for partial-thickness corneal transplantation. It involves removing the anterior layers of the cornea (the epithelium and the entire stroma) while preserving the patient’s own endothelium and Descemet’s membrane. These are the innermost and most fragile layers of the cornea.
The donor cornea is prepared so that only the matching anterior layers are transplanted. Unlike a full-thickness transplant (PKP or penetrating keratoplasty), DALK is a "selective" procedure because it only replaces the diseased tissue.
Indications
DALK is suitable for conditions where the endothelium remains healthy, specifically:
- Keratoconus: Advanced cases or those with stromal opacities.
- Stromal Scars: Whether superficial or deep, provided there is no endothelial damage.
- Stromal Dystrophies (E.g., granular, lattice, etc)
- Post-infectious Opacities: (e.g., from herpes or bacterial keratitis) if the endothelium is unscathed.
Benefits
- Endothelial Preservation: There is virtually no risk of endothelial rejection, which is the primary cause of long-term transplant failure.
- Lower Rejection Rates: The overall rejection rate is approximately three times lower than that of a full-thickness (PKP) transplant.
- Structural Integrity: The eye maintains better mechanical strength and is more resistant to future trauma.
- Long-term Stability: Reduced risk of corneal decompensation and a shorter requirement for topical immunosuppressants (steroid drops).
Risks and Complications
- Descemet’s Membrane Perforation: During dissection, the thin inner membrane may tear. Depending on the surgeon's experience, this occurs in 5–30% of cases and may require "conversion" to a full-thickness PKP.
- Minor Rejection: Epithelial or stromal rejection can occur, though these are usually easily treated and less serious than endothelial rejection.
- Postoperative Astigmatism: Like all transplants, the cornea may heal with an irregular shape, requiring spectacles, contact lenses and further surgical or laser refinement.
- Suture-related issues: Risks include infection, inflammation or loosening (dehiscence) of the stitches.
Contraindications
- Weakened Endothelium: Conditions like Fuchs’ Dystrophy or existing endothelial decompensation.
- Previous Intraocular Surgery: If prior procedures have significantly damaged the endothelial cell count.
- Deep Stromal Opacities: Scars that are so deep they are fused to Descemet’s membrane, often requiring conversion to PKP.
Technological Advancements: Femto-DALK
Femto-DALK is an evolution of the classic technique that uses a Femtosecond laser to perform high-precision cuts in both the recipient's cornea and the donor graft.
This technology allows for:
- Standardisation: Precise, personalised incisions with complex profiles (such as "mushroom" or "top hat" cuts).
- Improved Alignment: Better matching between the host and the graft, leading to a stronger wound junction and potentially better visual quality.
- Safety: By reducing manual dissection, it may lower the risk of accidental perforation of Descemet’s membrane and therefore conversion to PKP.
Conclusion
DALK is a sophisticated, modern transplant technique that effectively treats corneal pathologies while significantly reducing the long-term risk of rejection. It requires a detailed preoperative assessment by a cornea specialist and diligent postoperative care to ensure the best outcome.
Les différentes types de greffes
Découvrez les kératoplasties (= greffes de cornée)
Frequently asked questions
If you have any further questions, please do not hesitate to contact us!
Linked surgical treatments
Linked conditions
Book a consultation
Swiss Visio Montchoisi
1006 Lausanne, Switzerland