DWEK/DSO: Descemet’s Stripping Only
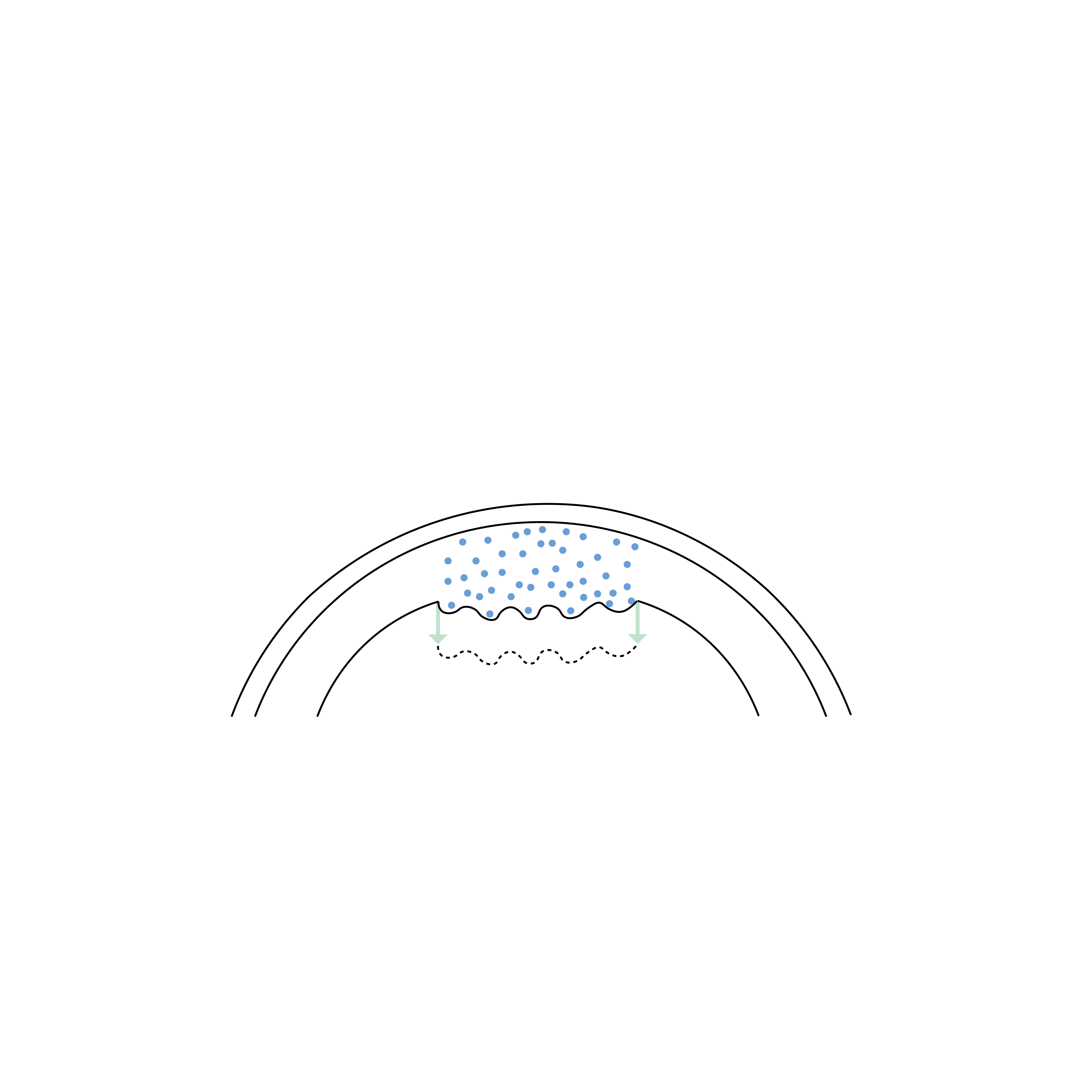
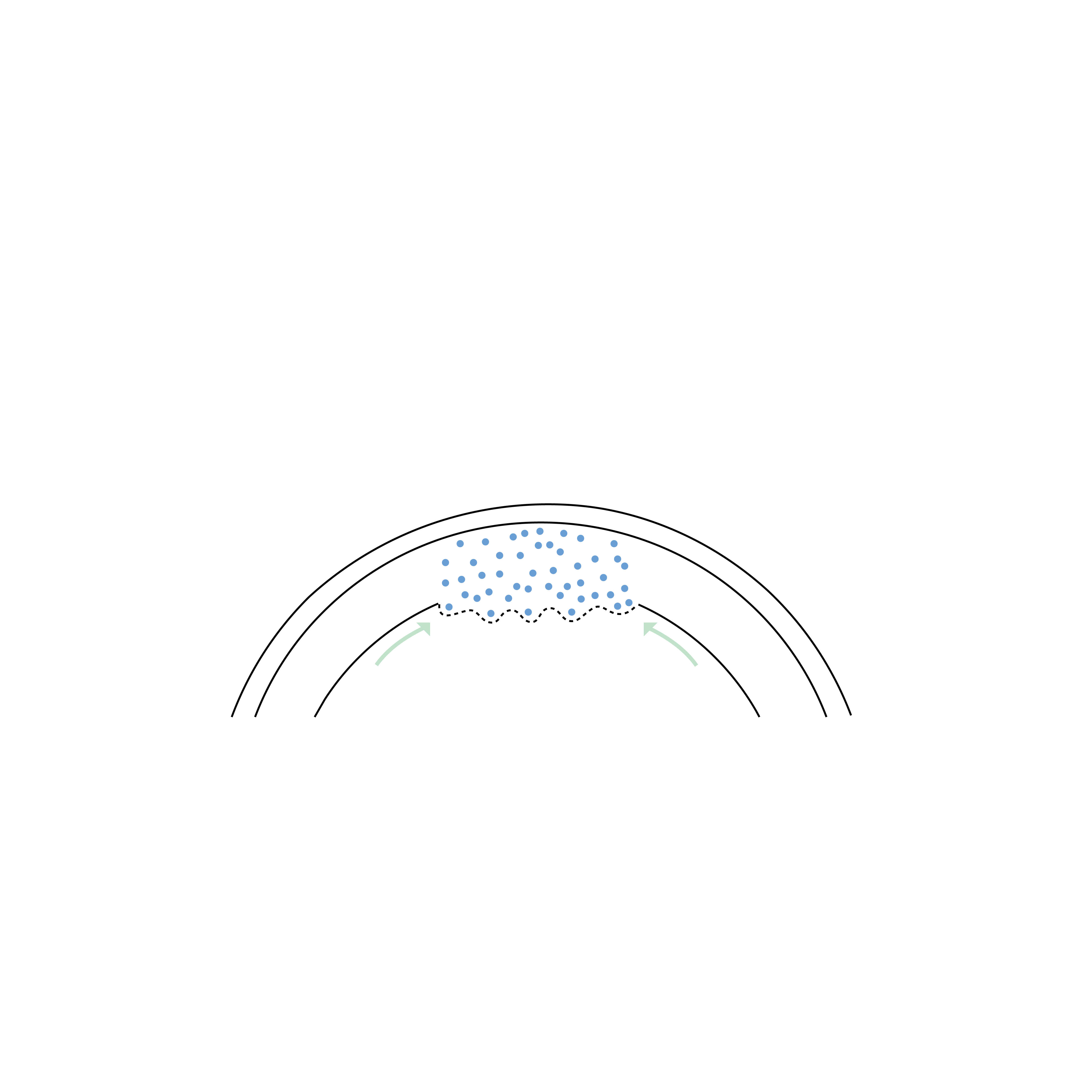
The DSO (Descemet's Stripping Only), also known as DWEK (Descemetorhexis Without Endothelial Keratoplasty), is a minimally invasive procedure used to treat Fuchs' endothelial dystrophy, a condition that leads to the deterioration of corneal endothelial cells and impaired vision. During DSO/DWEK, the surgeon removes the damaged central part of Descemet's membrane (a thin layer of the cornea) without replacing it with a donor graft, thereby allowing surrounding healthy endothelial cells to migrate and fill the gap, naturally restoring the endothelial pump function.


How does it work?
Learn more about the procedure / equipment
Why choose DSO over DMEK?
The reasons for performing Descemet's Stripping Only (DSO) are primarily related to conditions where the corneal endothelial cells — responsible for maintaining its transparency — become dysfunctional.
Here are the main indications for which DSO may be considered instead of an endothelial lamellar graft such as a DMEK:
Fuchs' Endothelial Corneal Dystrophy (FECD): DSO can be useful for treating mild to moderate forms of Fuchs' endothelial dystrophy, a genetic disease leading to progressive deterioration of corneal endothelial cells.
Localized Endothelial Dysfunction: Specific areas of the endothelial layer can be damaged due to trauma, disease, or previous surgical interventions.
Avoiding Graft Rejection: For patients at high risk of graft rejection or those with difficulty accessing donor tissue (e.g., due to immunological risks or logistical constraints), DSO avoids the need for corneal transplantation.
Who is not a good candidate for DSO?
Descemet's Stripping Only (DSO) is not suitable in certain situations where the natural migration of remaining endothelial cells would not allow for sufficient functional recovery, such as:
Fuchs' Endothelial Dystrophy advanced: When the density of remaining endothelial cells is too low, they cannot effectively migrate to restore corneal transparency. In these cases, an endothelial graft such as DMEK or DSAEK is preferable.
Diffuse Endothelial Failure: If the entire endothelium is severely affected, DSO would not be effective because there would not be enough healthy cells to recolonize the cornea.
Presence of Extensive Peripheral Guttae: If the guttata extends beyond the central zone and affects a large part of the cornea, cell migration will not be sufficient to restore normal endothelial function.
Older Patients with Low Cellular Regeneration Potential: The effectiveness of DSO relies on the ability of residual endothelial cells to migrate. In older patients, this ability is reduced, making the procedure less effective.
History of Multiple Intraocular Surgeries: After several intraocular interventions, the endothelium can be globally weakened, limiting the chances of recovery after DSO.
Endothelial Rejection or Failure of a Previous Corneal Graft: If a patient has already undergone an endothelial graft (DMEK, DSAEK) that failed due to immune rejection, DSO is not a viable option because the remaining endothelium is already non-functional.
In these situations, alternatives such as DMEK (Descemet’s Membrane Endothelial Keratoplasty) or DSAEK (Descemet’s Stripping Automated Endothelial Keratoplasty) are generally more appropriate, allowing for direct replacement of the deficient endothelium.
What are the risks and limitations of DSO?
Uncertain Visual Recovery: Unlike endothelial grafts (DMEK, DSAEK), DSO relies on the spontaneous migration of remaining endothelial cells. In some patients, this process may be insufficient, leading to incomplete or delayed visual recovery.
Persistent Corneal Edema: If endothelial repopulation is too slow or insufficient, the cornea may remain swollen (chronic edema), eventually requiring an endothelial graft (DMEK, DSAEK).
Variable Recovery Time: Recovery after DSO can be longer than that observed with an endothelial graft. Some patients regain functional vision within a few months, while others may need to wait 6 to 12 months for optimal recovery (vs DMEK recovery in a few days to a few weeks).
Risk of Corneal Opacification: If endothelial migration is insufficient, corneal transparency may not be fully restored, leading to a persistent decrease in vision.
Possibility of a Secondary Procedure: In case of DSO failure, an endothelial graft (DMEK or DSAEK) may be necessary, thus delaying definitive treatment and prolonging the period of reduced vision. In cases of prolonged edema, corneal scars may appear, subsequently requiring a full-thickness graft (PKP) to restore vision.
Les différentes types de greffes
Découvrez les kératoplasties (= greffes de cornée)
Frequently asked questions
If you have any further questions, please do not hesitate to contact us!
What is DSO/DWEK and how does it work?
DSO/DWEK is a minimally invasive corneal surgery that involves removing damaged endothelial cells and the affected portion of Descemet's membrane, without replacing them with donor tissue. Healthy cells located at the periphery of the cornea migrate to cover the treated area and restore corneal function.
Who is a good candidate for DSO/DWEK?
Candidates for DSO/DWEK are typically patients with mild to moderate Fuchs endothelial dystrophy or localized endothelial dysfunction, who have a sufficient number of healthy endothelial cells in the corneal periphery to restore corneal clarity.
How is DSO/DWEK different from endothelial corneal transplants (DMEK, DSAEK)?
DSO/DWEK does not require donor tissue, whereas DMEK and DSEK replace the damaged endothelial layer with a donor graft.



Linked conditions
Book a consultation
Swiss Visio Montchoisi
1006 Lausanne, Switzerland