DSAEK: Descemet's Stripping Automated Endothelial Keratoplasty
DSAEK (Descemet’s Stripping Automated Endothelial Keratoplasty)
DSAEK surgery involves inserting a thin layer of donor corneal tissue, approximately one-tenth of a millimeter thick (100 μm), containing healthy endothelial cells with their Descemet's membrane and corneal stroma, through very small incisions. The procedure is typically performed under local anesthesia, similar to cataract surgery.


How does it work?
Learn more about the procedure / equipment
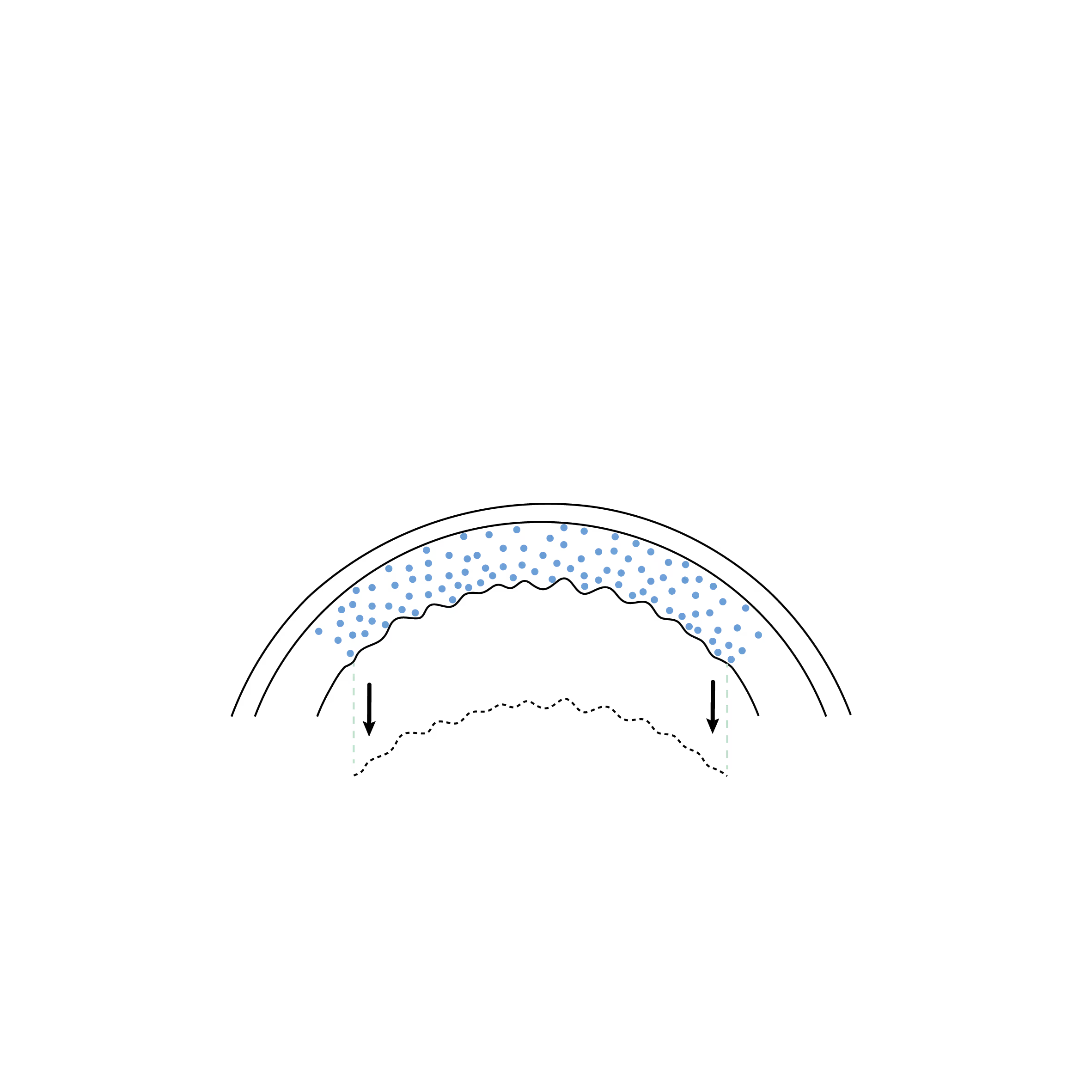
The patient's cornea is edematous, and their dysfunctional endothelium is removed through tiny incisions similar to those used for cataract surgery.
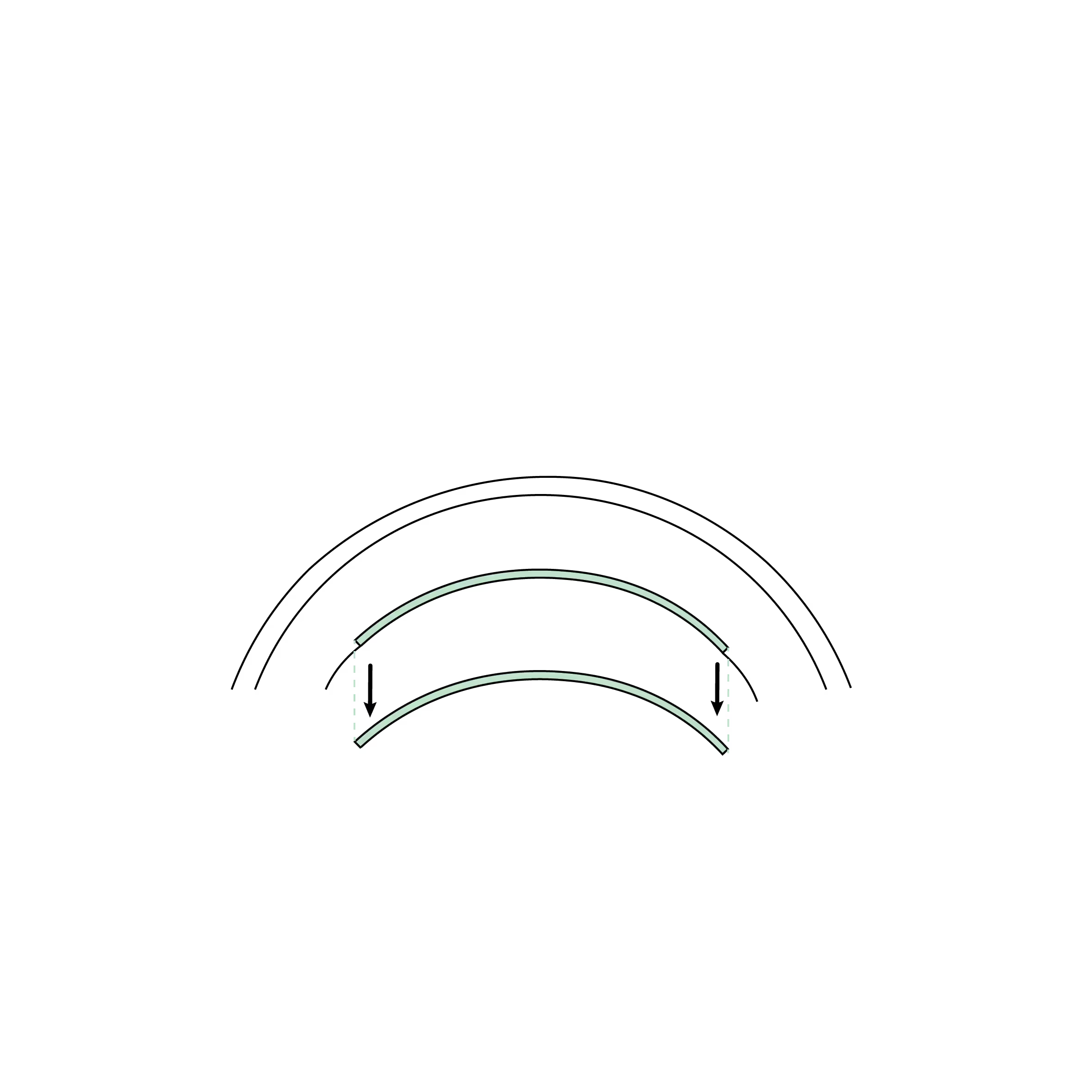
The DSAEK graft, containing the endothelium, Descemet's membrane, and a thin layer of stroma, is harvested from a donor cornea.
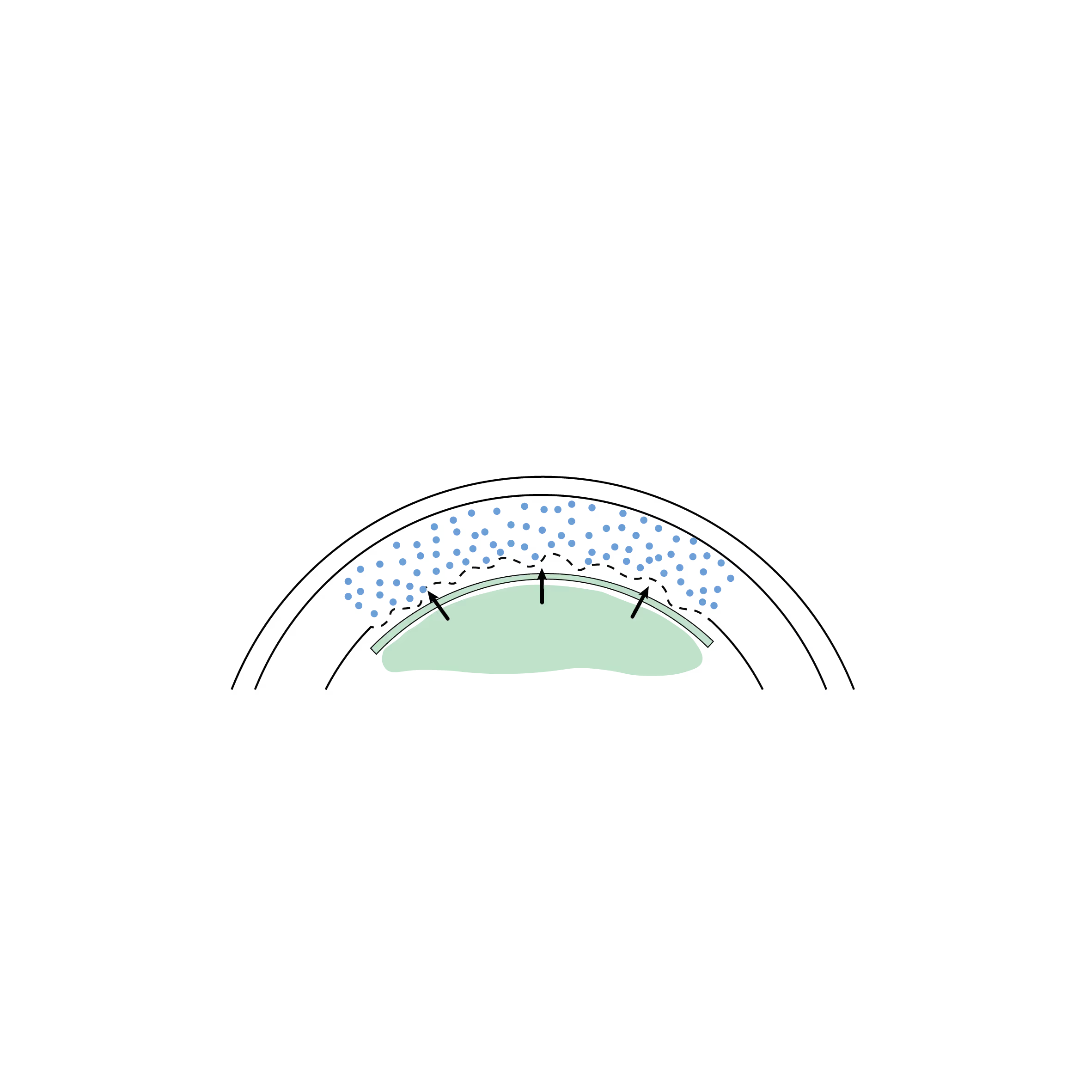
The DSAEK graft is inserted into the anterior chamber of the patient's (recipient's) eye, then positioned against the cornea using an air or gas bubble injected underneath, allowing it to appose and adhere to the posterior surface of the cornea.

Once the graft has adhered and endothelial pump function is restored, the cornea regains its transparency, thereby improving the patient's vision.
What is DSAEK?
DSAEK is a type of corneal transplant known as lamellar, which involves replacing only the damaged or diseased endothelial layer of the cornea with a thin layer of cornea containing stroma, Descemet's membrane, and endothelial cells from a donor graft.
DSAEK aims to restore vision by replacing endothelial cells, rather than the entire thickness of the cornea as in a penetrating keratoplasty (PKP). This approach allows for faster recovery and reduces the risk of complications associated with traditional corneal transplants.
DSAEK is generally reserved for complex situations where a DMEK is difficult to perform or has previously failed. However, advancements in DMEK surgical techniques allow it to be successfully performed in the majority of clinical scenarios, both simple and complex.
How is the procedure performed?
- Donor Tissue Preparation: A thin layer of healthy corneal tissue, containing the endothelium, Descemet's membrane, and part of the stroma, is prepared. This process is often automated to ensure precise and uniform graft thickness.
- Removal of Damaged Tissue: The surgeon removes the Descemet's membrane and diseased endothelial cells from the patient's cornea.
- Donor Graft Insertion: The prepared graft is gently folded and inserted into the eye through a small incision. Once inside, it is unfolded and positioned against the inner surface of the cornea.
- Graft Fixation: To keep the graft in place, an air or gas bubble is injected into the eye. This bubble applies pressure to the graft, helping it adhere to the existing corneal tissue. Patients are often advised to lie flat on their back for several hours to ensure proper graft fixation.
- Healing and Recovery: Recovery after DSAEK is faster than with traditional corneal transplants, as only a small part of the cornea is replaced. Full recovery can take a few months, with gradual vision improvement over time. However, recovery is slower than for DMEK.
What are the main benefits of DSAEK?
Selective Transplantation: Only the damaged inner layer is replaced, thus preserving the majority of the patient's cornea.
Rapid Recovery: Since DSAEK uses a smaller incision and replaces less tissue than a full-thickness corneal transplant , patients generally experience a shorter recovery time. Recovery after a DMEK is generally even faster, one of the reasons why DMEK has become the "Gold Standard" in terms of endothelial lamellar keratoplasty.
Reduced Risk of Complications: The smaller incision size reduces the risk of complications such as infection or wound dehiscence.
Reduced Risk of RejectionDSAEK has a lower rejection rate than penetrating keratoplasty but a higher rate than DMEK. The smaller the amount of foreign tissue transplanted, the less immune response there is (another reason why DMEK is favored).
Better structural integrityThe cornea retains its structural integrity, which reduces the risk of long-term complications such as astigmatism compared to full-thickness grafts.
What are the main indications?
- Fuchs' endothelial dystrophy (the most common)
- Endothelial decompensation or bullous keratopathy after intraocular surgery (e.g., cataract, glaucoma)
- Endothelial decompensation of a previous graft (e.g., after a PKP or a previous DSAEK)
- Iridocorneal Endothelial (ICE) Syndrome
- Isolated endothelial trauma
DSAEK is not recommended in cases of significant stromal corneal opacity, in which case PKP would be preferable.
Furthermore, in cases of high rejection risk or a history of multiple rejections, the implantation of an artificial "graft" such as Endoart may be more appropriate.
What are the risks and complications?
Although DSAEK is a proven and safe technique, it carries certain specific risks. The extensive clinical experience with this procedure now allows for very effective management of these eventualities.
1. Partial graft detachment (Rebubbling)
As with DMEK, the graft may not remain perfectly attached to the cornea in the first few days. However, since the DSAEK graft is thicker, it is often heavier and requires particular attention to the air/gas bubble.
- Treatment: A re-injection of an air or gas bubble ("rebubbling") is usually sufficient to stabilize the graft's position.
2. Immunological rejection
DSAEK carries a lower risk of rejection than a traditional corneal transplant (PKP), but higher than that of DMEK. This is due to the presence of a thin layer of stroma (foreign tissue) accompanying the endothelium.
- Statistics: The rejection rate in DSAEK is generally between 7% and 12% according to studies.
- Prevention: Regular follow-up and the diligent application of anti-rejection eye drops (e.g., corticosteroids, cyclosporine, tacrolimus) are the best guarantees to avoid this complication.
3. Primary or late graft failure
In rare cases, the donor endothelial cells fail to restore corneal transparency (primary failure) or their number decreases prematurely over time.
- Solution: If the cornea remains opaque after a few weeks, a graft replacement may be considered.
4. Other minor or rare risks
- Ocular hypertension: An increase in eye pressure may occur after the procedure, often related to eye drops or the gas bubble. It is usually well controlled with local medical treatment.
- Infection: This risk is rare due to the rigorous asepsis of the operating room.
- Cataract development: If the patient has not yet undergone cataract surgery, DSAEK can accelerate its development. A combined procedure is therefore frequently recommended in such cases.
Les différentes types de greffes
Découvrez les kératoplasties (= greffes de cornée)
Frequently asked questions
If you have any further questions, please do not hesitate to contact us!
How is DSAEK surgery performed?
The surgeon removes the damaged endothelial layer (Descemet's membrane) through a small incision and inserts the prepared donor tissue. The graft is positioned using an air or gas bubble, which holds it in place until it naturally adheres.
What is the recovery time after a DSAEK?
Visual improvement begins within a few days to a few weeks, but full recovery can take several months as the graft fully integrates.
How long does the DSAEK procedure last?
The procedure usually lasts between 30 and 60 minutes.





Book a consultation
Swiss Visio Montchoisi
1006 Lausanne, Switzerland