DMEK: Ultra-Thin Endothelial Transplant
DMEK (Descemet's Membrane Endothelial Keratoplasty)
During DMEK surgery, the diseased endothelium is removed and replaced with a single layer of donor endothelial cells, barely a hundredth of a millimeter thick.
The main advantages of DMEK include faster visual recovery compared to DSAEK and a rejection rate of less than 1% (which is about 10 times lower than for DSAEK).
However, not all patients are ideal candidates for this technique, and your surgeon will discuss it with you. The procedure is generally performed under local anesthesia, similar to cataract surgery, and lasts between 30 minutes and 1 hour, depending on the complexity of the operation.


How does it work?
Learn more about the procedure / equipment
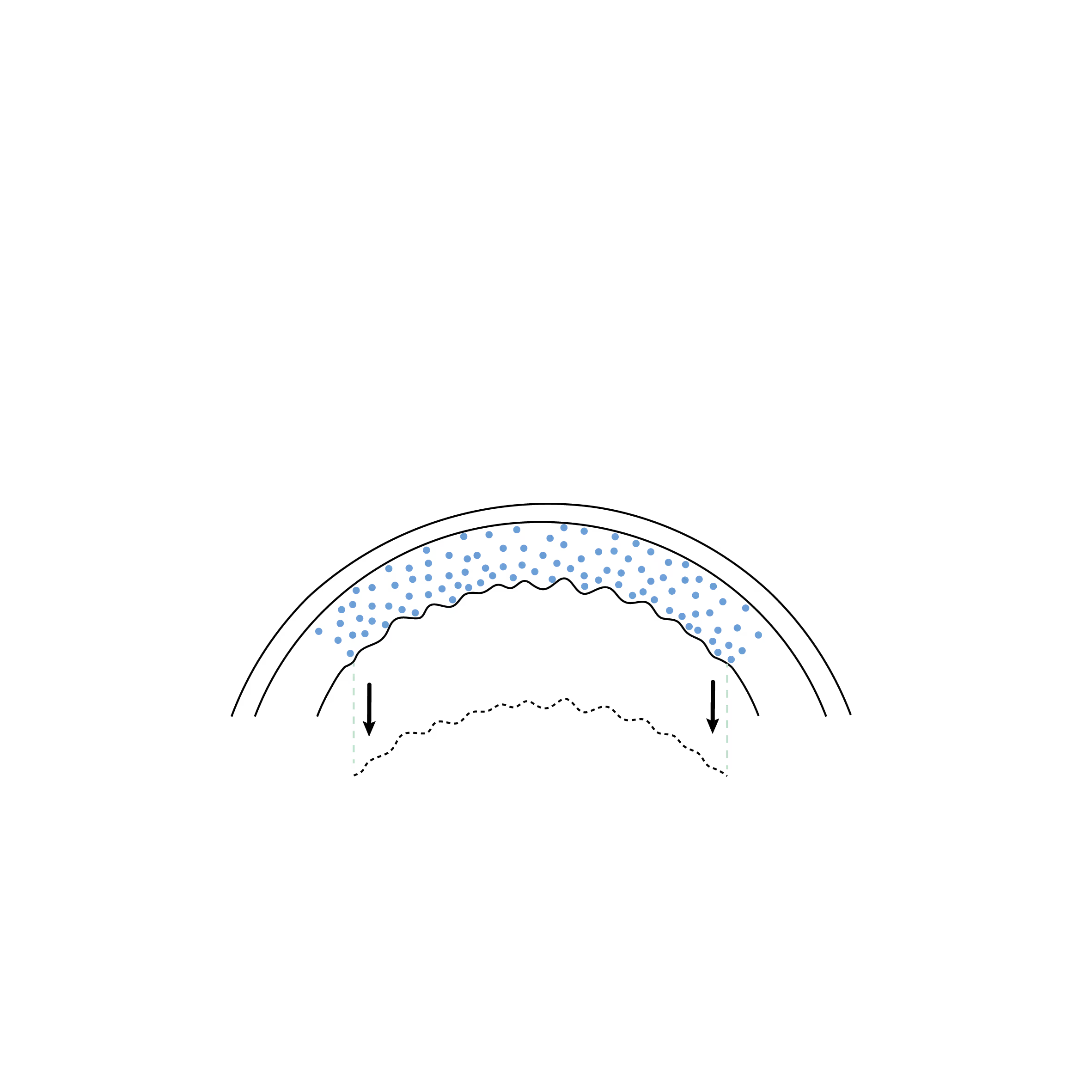
The patient's cornea is edematous, and their dysfunctional endothelium is removed through tiny incisions similar to those used for cataract surgery.

The DMEK graft, containing only the endothelium and its Descemet's membrane, is delicately harvested from a donor cornea.
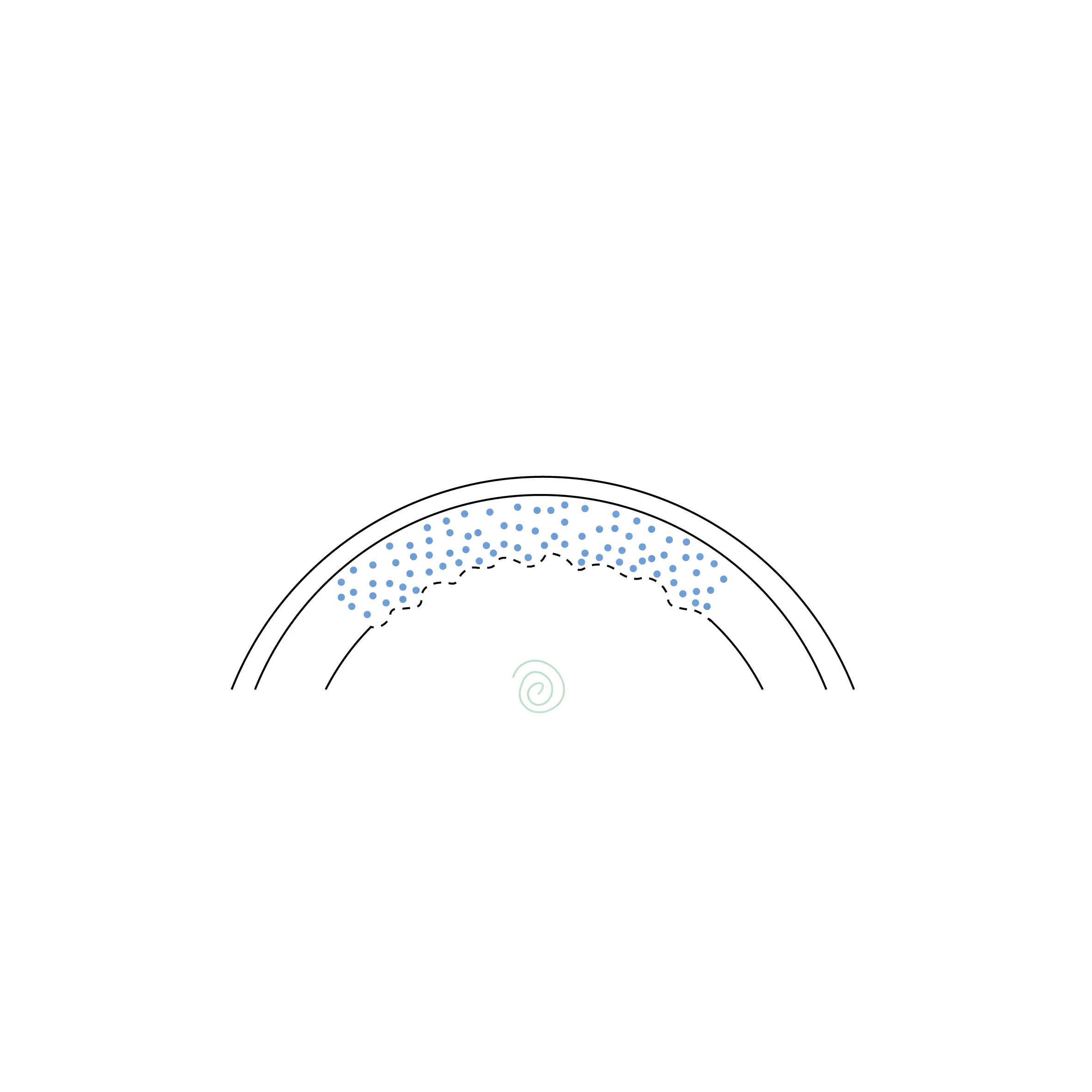
The DMEK graft is a very thin membrane that naturally curls up like parchment paper. It is injected into the eye through a small incision to replace the diseased layer.
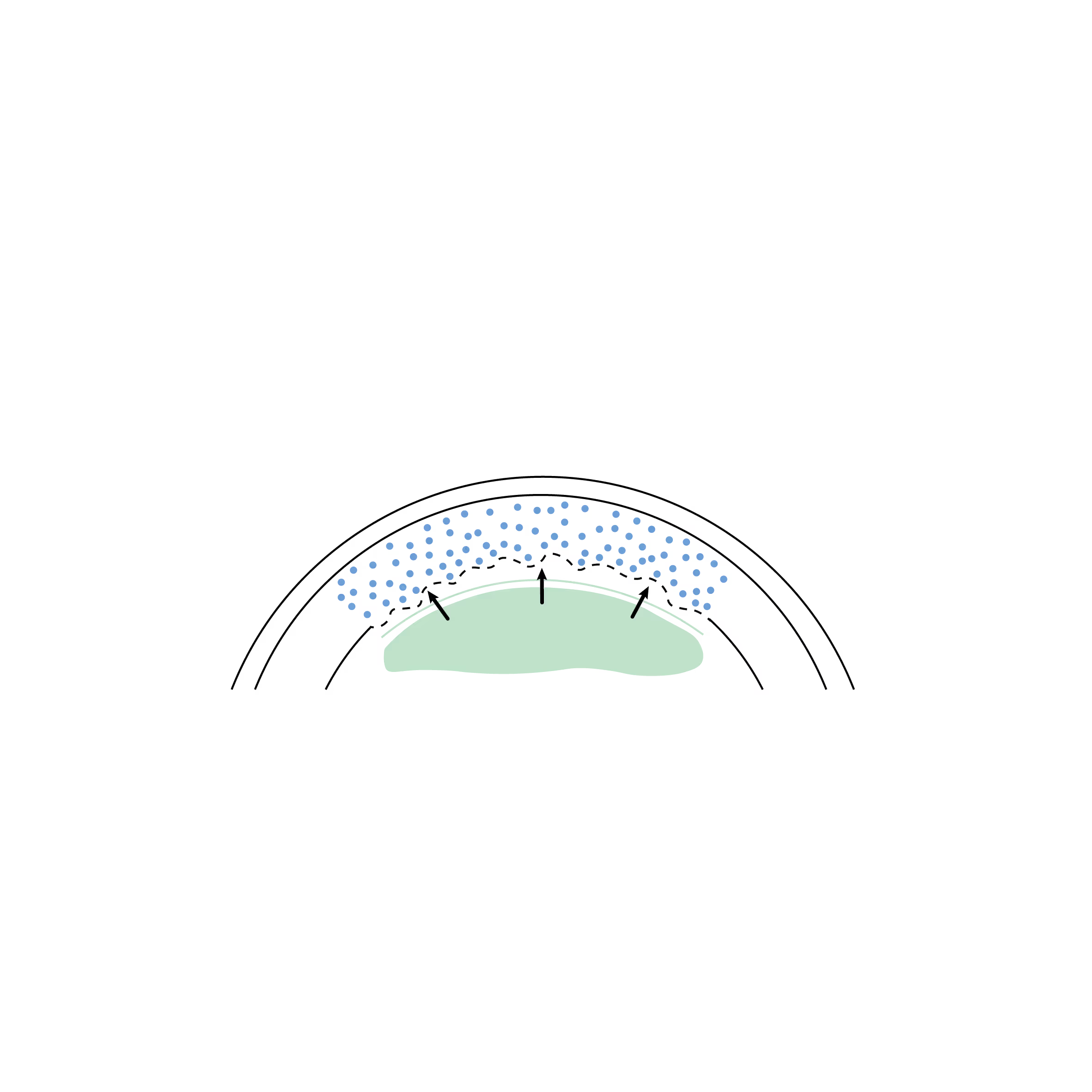
The DMEK is carefully unfolded inside the eye, then an air or gas bubble injected underneath presses the graft against the inner surface of the cornea. It adheres naturally, like a sticker, without the need for sutures.

DMEK integrates into the cornea and restores the endothelial pump function, allowing excess fluid to drain. The cornea then regains its transparency, and vision improves.
What is DMEK?
The Keratoplasty Endothelial of the Membrane of Descemet (DMEK) is an extremely advanced and precise corneal transplant technique that involves replacing only the damaged endothelial layer of the cornea. This endothelial layer is essential for maintaining corneal clarity by pumping out excess fluid.
DMEK is an ultrathin and precise graft that replaces only Descemet's membrane (a thin layer that supports the endothelial cells and separates them from the stroma) as well as the endothelial cells, making it even more selective than DSAEK (Descemet’s Stripping Automated Endothelial Keratoplasty).
The surgical advancements and innovations of modern DMEK make it the procedure of choice for most clinical situations requiring endothelial cell replacement. In rare cases where DMEK is difficult to perform or has failed, then a DSAEK becomes the second-choice procedure.
What is the procedure?
- Donor tissue preparation: The donor tissue for DMEK is an extremely thin graft, composed solely of Descemet's membrane and its attached endothelial cells. This graft is typically 10 to 15 microns thick, making it the thinnest corneal graft available. Preparing this tissue is therefore more delicate than for DSAEK and requires advanced expertise in corneal surgery.
- Removal of damaged endothelium: The surgeon removes Descemet's membrane and the damaged endothelial cells from the patient's recipient cornea through small incisions (similar to those used for cataract surgery).
- Insertion of the donor graft: The prepared graft is rolled up and inserted into the eye through one of these small incisions. Once inside the eye, it is gently unrolled onto the inner surface of the cornea.
- Graft fixation: To ensure the graft adheres to the patient's cornea, the surgeon injects an air or gas bubble into the eye, which presses the new membrane against the inner surface of the patient's cornea, allowing the graft to adhere well.
- Healing and recovery: Recovery after DMEK is generally rapid, taking a few days to a few weeks, with an earlier return to clear vision compared to other types of endothelial grafts such as DSAEK. Follow-up visits are essential to monitor graft adherence, proper function, and absence of rejection.
What are the benefits of DMEK?
- Selective and precise transplantation: Unlike DSAEK, which replaces both Descemet's membrane and part of the corneal stroma, DMEK only replaces Descemet's membrane and the endothelium. This makes it the most anatomically precise corneal transplant procedure.
- Faster and Higher-Quality Visual Recovery: Since less tissue is transplanted and the cornea retains more of its natural structure, patients generally experience faster visual recovery and better overall vision quality.
- Reduced Rejection Risk: DMEK has the lowest rejection rate among corneal transplant techniques. The reduced amount of foreign tissue transplanted lowers the risk of an immune response.
- Minimal Induced Astigmatism: Minimal manipulation of the cornea's shape during DMEK significantly reduces, or even almost entirely eliminates, the risk of inducing irregular astigmatism, which can occur with other corneal transplant procedures such as PKP, DALK and DSAEK.
What are the main indications?
Fuchs' Endothelial Dystrophy: This is the most common indication for DMEK. Fuchs' dystrophy is a genetic condition leading to a progressive loss of endothelial cells, causing swelling and gradual opacification of the cornea. As the disease progresses, patients experience blurred vision, especially in the morning, glare sensitivity, and significant vision loss in advanced stages.
Pseudophakic Bullous Keratopathy: This condition occurs when endothelial cells are damaged after cataract surgery. The cornea swells and forms blisters (epithelial bullae), leading to pain and decreased vision. DMEK is often the best treatment to restore vision and comfort for these patients.
Traumatic Corneal Endothelial Lesions: Ocular trauma, including surgical trauma, can damage endothelial cells, leading to corneal swelling and decreased vision. DMEK can be used to replace the damaged endothelium.
Failure of a previous corneal transplant: If a patient has previously undergone a penetrating keratoplasty (PKP) or an endothelial lamellar keratoplasty (DSAEK, DLEK) and the grafted endothelial cells fail, a DMEK can be performed to replace only the endothelial layer, thus avoiding a full corneal transplant.
Congenital Hereditary Endothelial Dystrophy (CHED): This is a rare genetic disease affecting the endothelium from birth, leading to corneal opacification and visual impairment in children or young adults. DMEK can be an effective treatment to restore clarity and vision in affected individuals.
Iridocorneal Endothelial Syndrome (ICE): A rare condition affecting both the corneal endothelium and the iris, leading to progressive corneal swelling and decreased vision. DMEK may be recommended to replace the damaged endothelium in this disease.
What are the risks and complications?
Although DMEK is currently the safest and least invasive corneal transplant technique, it carries, like any surgical procedure, certain risks. The majority of these complications are manageable and do not alter the final visual outcome if treated promptly.
1. Partial graft detachment (Rebubbling)
This is the most common complication in endothelial surgery. Since the graft is extremely thin, it sometimes happens that a part of it does not remain perfectly adhered to the cornea in the days following the procedure.
- Medical reference: The scientific literature reports a detachment rate varying between 10% and 25% depending on the centers.
- Treatment: A simple re-injection of an air or gas bubble (a procedure called "rebubbling"), performed in a few minutes, allows the graft to reattach to the patient's cornea to ensure optimal adhesion.
Surgical expertise: Thanks to a rigorous technique, the "rebubbling" rate performed by Dr. Hammer over the last three years is less than 5%, a significantly better result than the average observed in the literature.
2. Immunological rejection
The risk of rejection is significantly reduced with the DMEK technique (less than 1%) compared to other types of grafts (DSAEK 7-12%, PKP > 15%), because very little foreign tissue is transplanted.
- Prevention: The rigorous instillation of prescribed anti-rejection eye drops (e.g., corticosteroids, cyclosporine, tacrolimus) is essential to prevent this risk in the long term.
3. Primary graft failure
In rare cases (1-2%), the graft may not function (the cells do not "pump" out the edema).
- Solution: A new graft may be necessary if the cornea does not clear after several weeks.
4. Other minor or rare risks
- Ocular hypertension: This is a temporary increase in eye pressure, often related to the use of eye drops or the presence of the gas bubble. It is usually well controlled with local medical treatment (drops).
- Infection: An exceptional risk thanks to rigorous sterility protocols.
- Development of cataract: If your eye has not yet undergone cataract, the graft procedure can sometimes accelerate its development. For this reason, and to ensure complete visual rehabilitation, combined surgery (DMEK + Cataract) is frequently offered when the lens already shows signs of opacification.
Les différentes types de greffes
Découvrez les kératoplasties (= greffes de cornée)
Frequently asked questions
If you have any further questions, please do not hesitate to contact us!
What is DMEK and why is it performed?
DMEK is a type of corneal transplant in which only the innermost layer of the cornea, consisting of Descemet's membrane and endothelial cells, is replaced. It is performed to treat conditions affecting the endothelium, such as Fuchs' endothelial dystrophy or corneal edema.
How long does the DMEK procedure take?
The procedure generally lasts between 30 and 60 minutes, depending on the specific characteristics of your eye and the complexity of the surgical technique.
Will I be awake during DMEK surgery?
Most DMEK procedures are performed under local anesthesia with sedation, but general anesthesia can be used if necessary.





Book a consultation
Swiss Visio Montchoisi
1006 Lausanne, Switzerland