Keratoconus
Keratoconus is a progressive eye condition that alters the shape of the cornea, resulting in blurred and distorted vision.
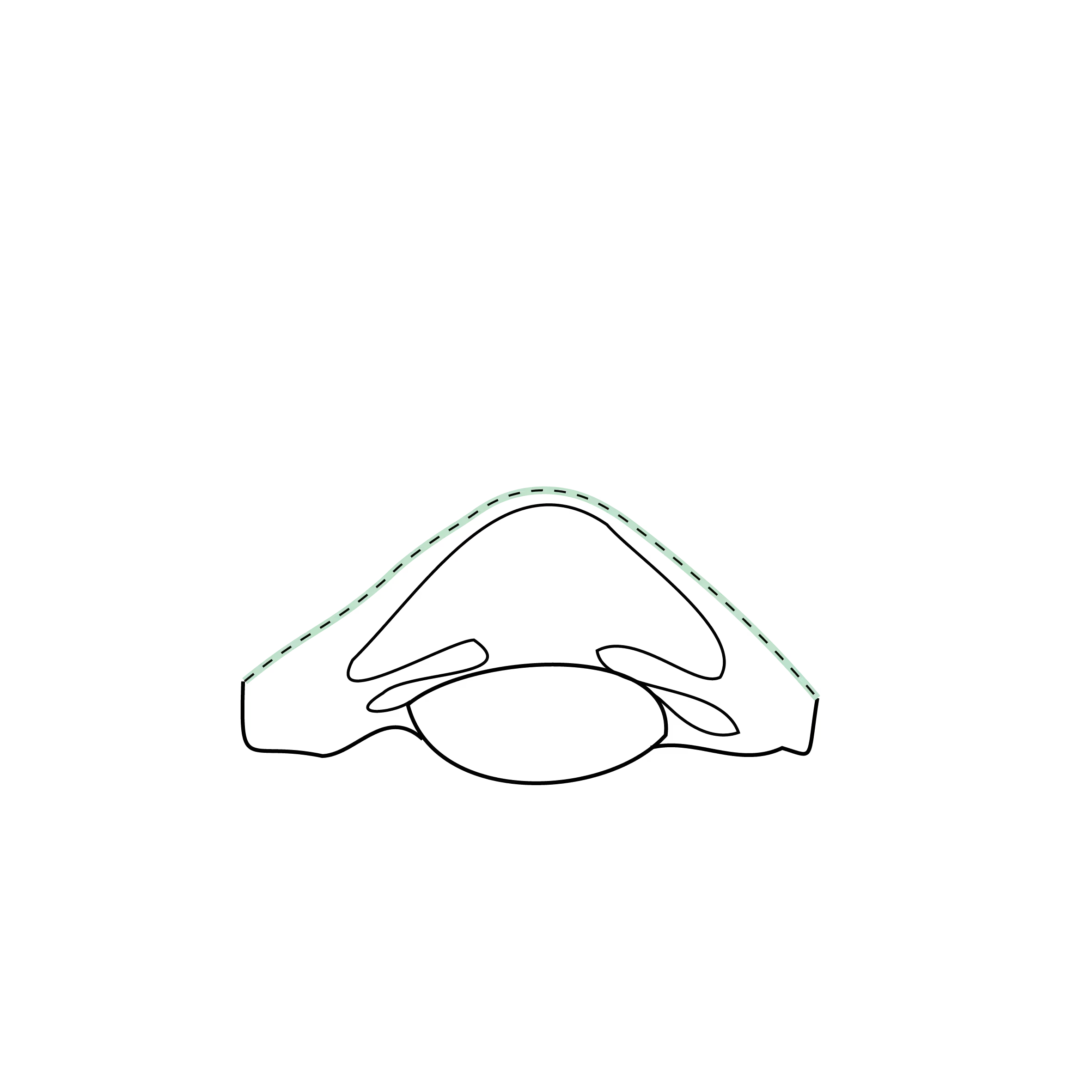
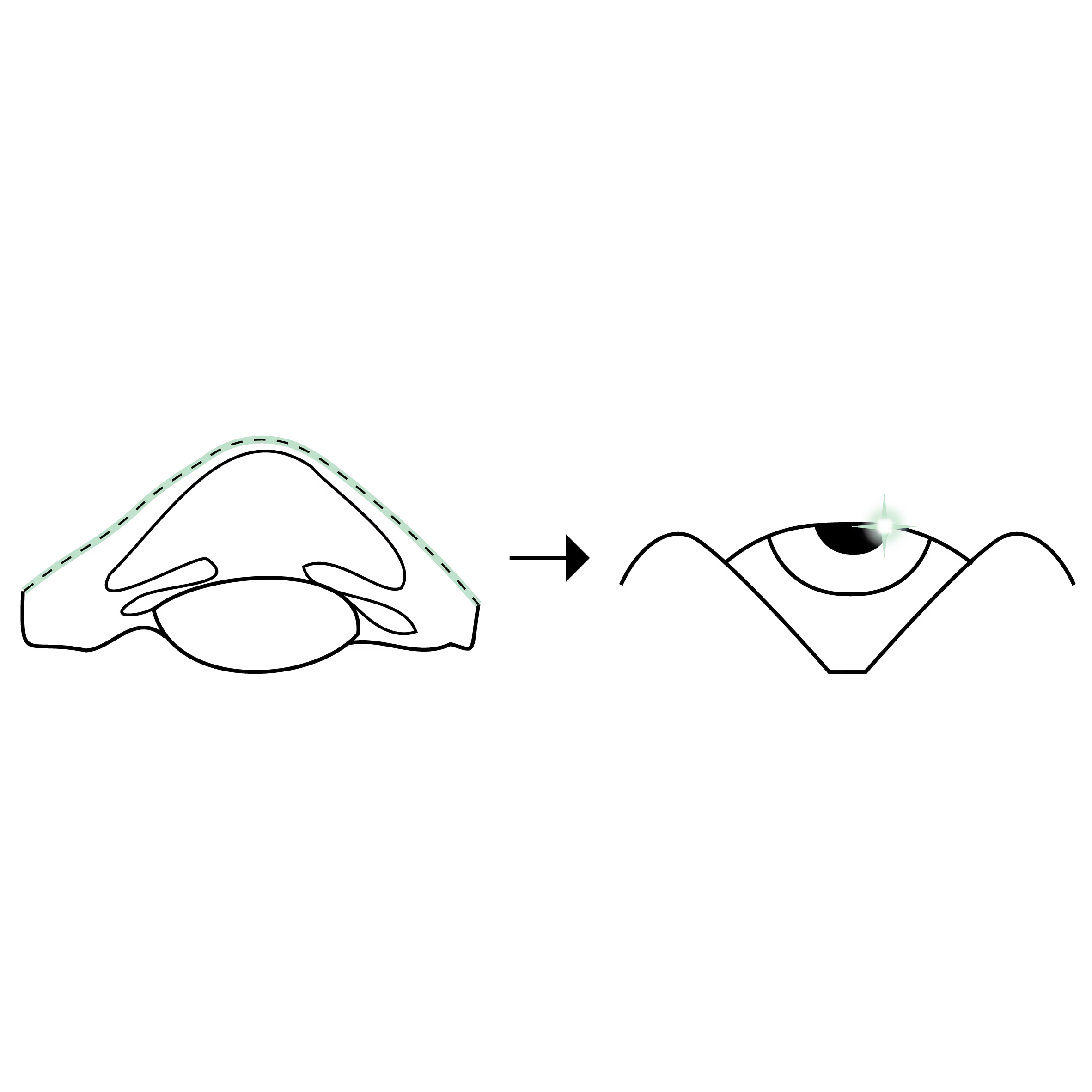
The condition is most likely to progress in younger patients and those who frequently rub their eyes, leading to a gradual thinning and weakening of the corneal tissue. This causes the cornea to develop an irregular, cone-shaped bulge, which impairs visual clarity.
If you have any questions regarding keratoconus or the available treatment options, please do not hesitate to contact us or book a consultation.

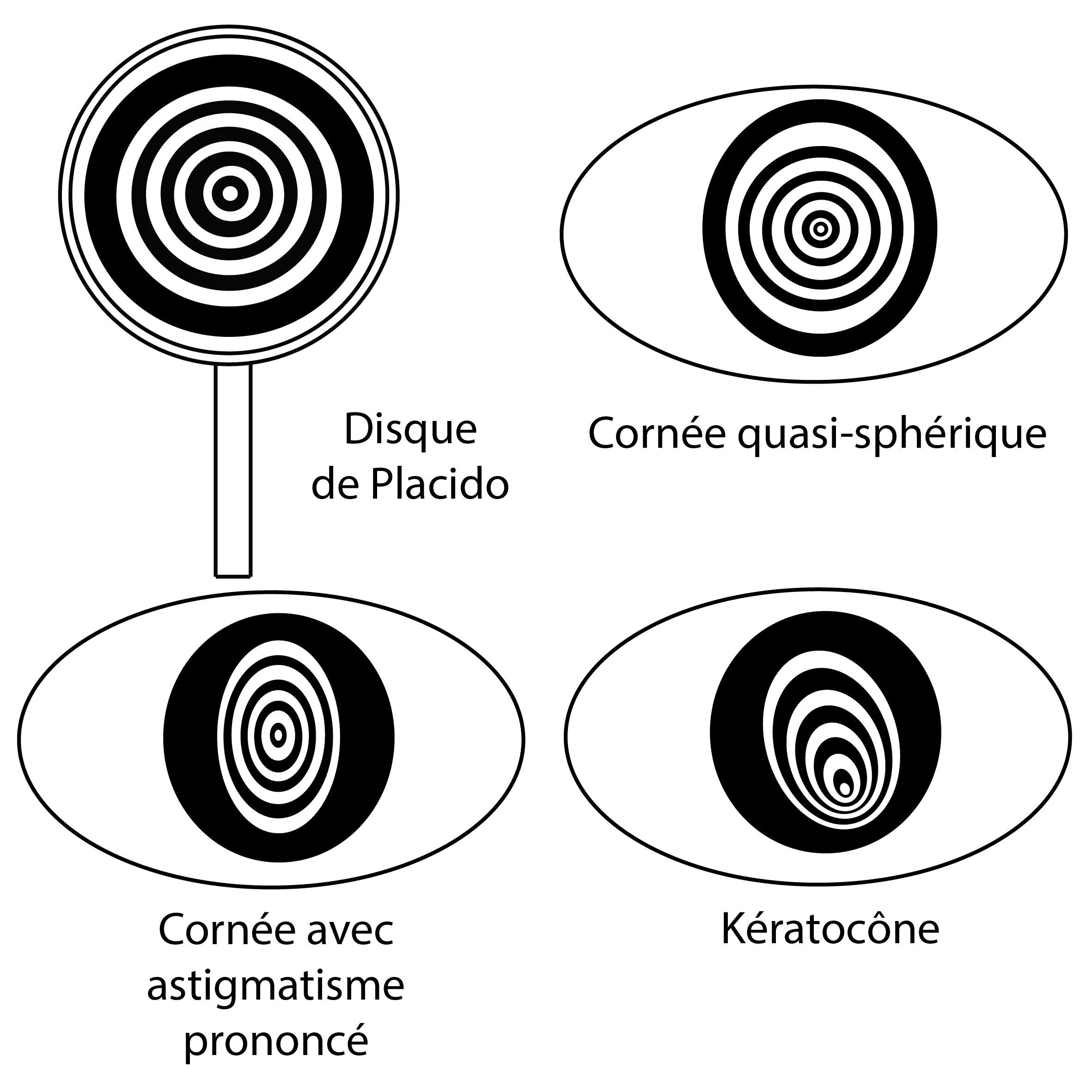
This image illustrates how light is reflected on the cornea according to its shape. On a normal cornea, the rings are regular. In the case of keratoconus, these rings become more and more irregular and stretched. The analysis of these reflections makes it possible to detect and monitor the evolution of keratoconus.
What is keratoconus?
Keratoconus is a progressive, non-inflammatory condition affecting the cornea (the clear front window of the eye). It causes the cornea to thin and develop a conical protrusion, altering how light enters the eye and resulting in distorted vision.
As the condition advances, the inner surface of the cornea can occasionally rupture, a phenomenon known as acute corneal hydrops.
What are the clinical characteristics?
Keratoconus generally affects both eyes, though the severity often varies between them. Opticians and optometrists may detect the condition by noting an increase in astigmatism. Any unexplained increase should prompt a referral for a medical evaluation, ideally by an ophthalmologist specialising in corneal disease.
Astigmatism caused by keratoconus is typically irregular, meaning it cannot be fully corrected with standard glasses. While mild or early cases may still achieve good vision with spectacles, advanced cases usually require special contact lenses to achieve optimal visual acuity.
What are the symptoms?
- Blurred and distorted vision: Making daily tasks like reading and driving more difficult.
- Sensitivity to light and glare: Particularly noticeable when driving at night.
- Frequent changes in prescription: If your spectacles or contact lens prescription changes regularly, it could be a sign of keratoconus.
- Double vision (ghosting): Often experienced in one eye.
What are the causes?
The condition stems from a structural and biomechanical weakness in the collagen and proteoglycan fibres that support the cornea. Keratoconus primarily affects individuals between adolescence and their early thirties.
Statistics and Risk Factors:
- Demographics: It is significantly more common in individuals with Down’s syndrome (Trisomy 21) and those with atopic conditions like asthma or eczema.
- Ethnicity: Research suggests higher prevalence rates in certain populations; for instance, studies in the UK have indicated a higher incidence in Asian (specifically Indian, Pakistani, and Bangladeshi) communities compared to Caucasian populations (approx. 4 to 1 ratio in some clinical audits).
- Triggers: Key factors include genetics, allergies, and eye rubbing.
How is keratoconus diagnosed?
Diagnosis is achieved using corneal topography or tomography (e.g. Placido, anterior segment OCT or Scheimpflug imaging). These technologies map the corneal surface to reveal irregular astigmatism and can detect subclinical forms (keratoconus fruste), which is vital before considering any laser refractive surgery. Regular check-ups are essential to monitor the speed of progression.
What are the treatments?
1. Medical Care
The most critical step is to stop rubbing the eyes. Recurrent, vigorous eye rubbing is a proven cause of corneal thinning and ectasia. Allergies and eye inflammation should be managed to maintain a healthy ocular surface and reduce the urge to rub.
2. Optical Support
- Glasses and soft contact lenses: Effective for mild cases.
- Special lenses: For moderate to advanced cases, scleral or hybrid contact lenses are used to provide a smooth optical surface, significantly improving vision.
3. Surgical Care
- Corneal Collagen Cross-linking (CXL): A procedure that strengthens the cornea to slow or stop progression.
- Corneal Regularisation: Combining (Trans) PRK (topography- or wavefront-guided) with CXL and/or using intracorneal rings/segments (CAIRS/ICRS).
- Keratoplasty (Corneal Transplant): Techniques such as DALK (Deep Anterior Lamellar Keratoplasty) or PKP (Penetrating Keratoplasty) are used when the cornea can no longer be managed by other means.
Alternative options when contact lenses are not suitable
If contact lenses cannot be tolerated, vision with glasses can often be improved by "regularising" the cornea through:
- Intracorneal rings/segments (CAIRS/ICRS): Synthetic (e.g. Keraring) or biological (CAIRS) segments inserted into the cornea.
- Excimer Laser Treatments: Such as Trans-PTK or topography-guided PRK, always combined with CXL.
Can I reduce my dependence on glasses?
In specific stable cases, an implantable contact lens (ICL/IPCL), also known as a phakic intraocular lens, can be surgically inserted to reduce the need for glasses or contact lenses.
What if none of this works for me?
In this type of situation, a corneal transplant (DALK, PKP) may be needed to replace a cornea that is too damaged to be regularised.
Corneal transplantation can also benefit from the visual rehabilitation procedures listed in the previous points:
- Special contact lenses to correct shape irregularities.
- Transplant regularisation treatments (TransPTK, TransPRK topo- or wavefront-guided) for patients who are intolerant of contact lenses in order to improve vision with spectacles.
- Implantable contact lenses to reduce dependence on glasses and contact lenses.
Motifs de consultations associés
Les procédures chirurchicales associées
.avif)
.avif)

.avif)
Les questions fréquentes
Si vous avez d'autres questions n'hésitez pas à nous contacter !
Book a consultation
Swiss Visio Montchoisi
1006 Lausanne, Switzerland