Keratoconus surgery
Keratoconus surgery keratoconus involves several different surgical options to manage or correct this progressive eye disease, characterized by a thinning and cone-shaped deformation of the cornea (the transparent layer at the front of the eye).
This irregular shape leads to distorted vision and difficulties performing tasks such as reading or driving.
Keratoconus treatment depends on the severity and progression of the disease, ranging from minimally invasive procedures to more complex surgeries.

How does it work?
Learn more about the procedure / equipment
Surgical Options for Keratoconus Management
Corneal Collagen Cross-linking (CXL): Strengthens and stabilizes corneal collagen fibers to slow or halt the progression of keratoconus, particularly useful in early stages.
ICRS (Intrastromal Corneal Ring Segments): Synthetic ring-shaped implants inserted into the cornea to flatten and reshape it, reducing astigmatism and improving vision.
CAIRS (Corneal Allogenic Intrastromal Ring Segments): An innovative technique using rings made from corneal tissue to reshape the cornea. These biological rings allow for better integration into the cornea and reduce the risk of complications compared to ICRS.
Laser corneal reshaping (transPTK/Topo- or wavefront-guided PRK) combined with CXL: Combines laser corneal reshaping for a more regular surface with crosslinking to stabilize the cornea and prevent progression.
Corneal Transplant (Keratoplasty): Replacement of the deformed cornea, either full-thickness with a penetrating keratoplasty (PKP), or replacement of the outer layers while preserving the endothelium with a Deep Anterior Lamellar Keratoplasty (DALK).
Implantable Contact Lenses (ICL/IPCL): Complement the treatment to provide better visual acuity when glasses or contact lenses are no longer tolerated or sufficient.
Each technique is chosen based on the degree and progression of keratoconus, as well as the patient's needs.
CXL: How does it work?
CXL (Corneal Collagen Cross-linking) is a treatment designed to strengthen and stabilize the corneal structure to halt the progression of keratoconus, especially in its early stages.
Procedure:
- The eye is anesthetized with anesthetic drops, and the superficial layer of the cornea (epithelium) is sometimes removed (in "epithelium-off" procedures).
- Riboflavin (vitamin B2) drops are applied to the cornea, followed by exposure to ultraviolet (UV) light.
- Riboflavin, activated by UV light, strengthens the collagen fibers in the cornea by creating new bonds between molecules.
Benefits: CXL is minimally invasive and effective in slowing or stopping the progression of keratoconus in most cases, thereby reducing the need for more invasive surgeries.
Limitations: Although it stabilizes the cornea, it does not significantly improve vision; other treatments can be combined with CXL to enhance vision.
Laser corneal remodeling combined with CXL: how does it work?
Objective:
- This procedure combines excimer laser treatments, which reshape the cornea to make it less irregular, with crosslinking, which stiffens the cornea.
- This allows for simultaneous improvement of vision and stabilization of the cornea.
- The goal here is to improve spectacle-corrected vision for patients who cannot use contact lenses.
Procedure:
- Corneal remodeling uses an excimer laser to remove small amounts of corneal tissue to make the surface smoother and more regular. This can be done with different modalities such as TransPTK and topography-guided PRK or ocular aberration-guided PRK. These are "customized" methods specific to the patient's cornea.
- These combined treatments improve vision quality and strengthen/stabilize the cornea to prevent keratoconus progression in a single procedure.
Limitations:
- Vision improvement may be limited. This option is generally used for mild to moderate keratoconus.
- The purpose of these treatments is not to reduce dependence on glasses but to improve spectacle-corrected vision.
- Once the cornea is satisfactorily regularized, it is possible to reduce dependence on glasses thanks to implantable contact lenses (ICL/IPCL).
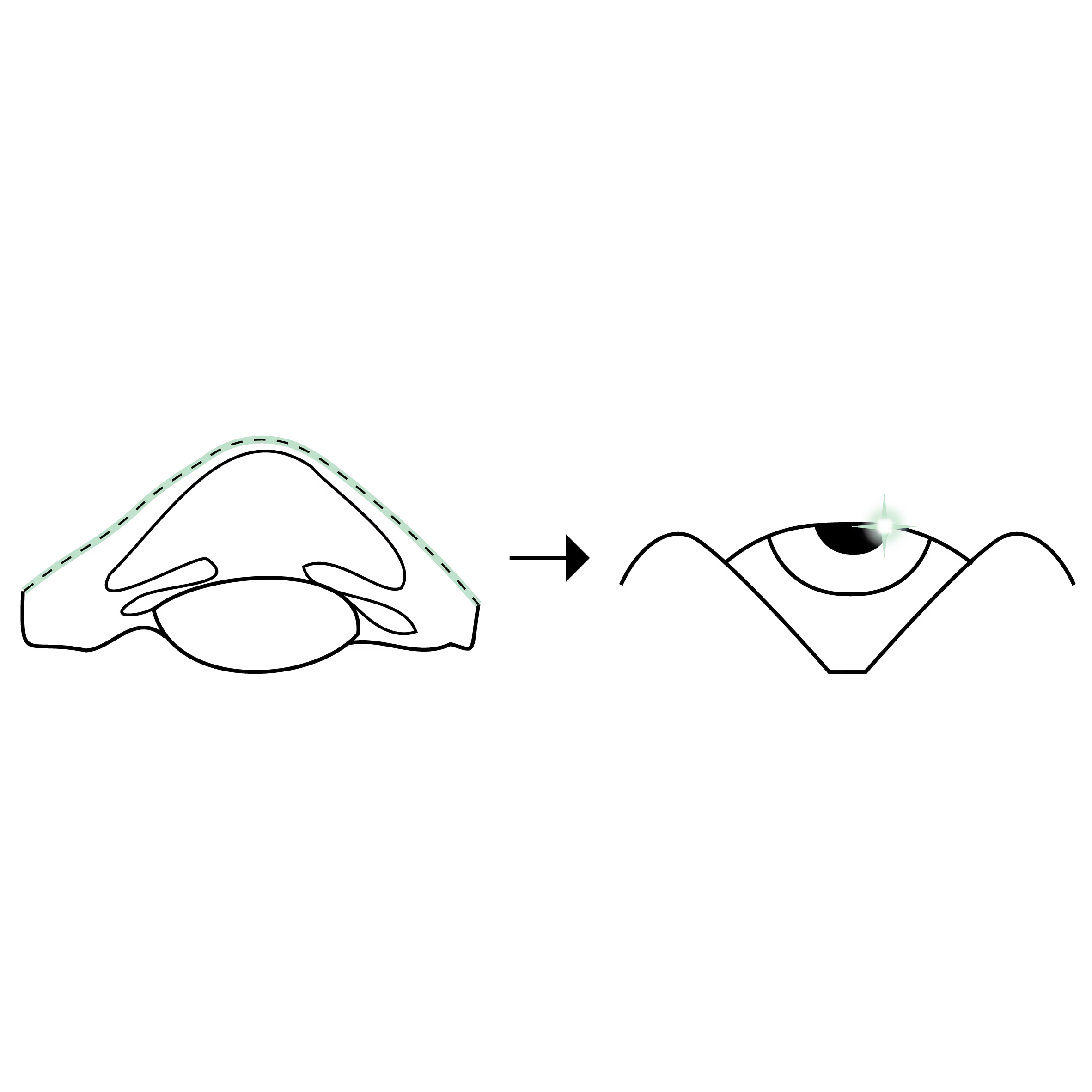
Intracorneal segments (ICRS/CAIRS): How do they work?
Intracorneal segments can be synthetic (ICRS) or biological (CAIRS). They reshape and regularize the cornea to improve vision quality.
Procedure:
- A small incision and channels are precisely shaped inside the cornea using a femtosecond laser, and thin synthetic (ICRS) or biological (CAIRS) crescent-shaped segments are inserted.
- These segments act as internal reinforcements, giving the cornea a more regular shape.
Advantages:
- Intracorneal segments can improve vision by regularizing the cornea. They are also reversible if necessary and are generally used in cases of moderate to severe keratoconus where the cornea is too irregular and/or too thin for combined excimer laser treatments (TransPTK / Topography- or wavefront-guided TransPTK) with CXL.
- Intracorneal segments can be combined with CXL in the same procedure for patients with progressive keratoconus.
Limitations:
- Not all patients are eligible for synthetic segments (ICRS) because the cornea must have a minimum thickness to safely insert them and avoid surface exposure or penetration into the eye.
- Biological segments (CAIRS), on the other hand, have less strict criteria, making more patients eligible. Being biological, they integrate more readily with the cornea and present fewer risks of complications such as spontaneous extrusion.
Corneal Transplants: How do they work?
When keratoconus is at an advanced stage and vision cannot be corrected by other methods, a corneal transplant may be necessary. There are two types:
- Penetrating Keratoplasty (PKP): Full-thickness transplant, where the entire deformed and/or opacified area of the cornea is replaced.
- Deep Anterior Lamellar Keratoplasty (DALK): Only the surface and intermediate layers of the cornea are replaced, which reduces the risk of rejection.
Procedure:
- The diseased cornea is carefully removed and replaced with a donor cornea, which is secured with sutures.
Advantages:
- Corneal transplants are very effective in restoring vision in advanced keratoconus cases. The DALK has a lower rejection rate than PKP.
- When a keratoconus-affected cornea is replaced with a corneal transplant, visual rehabilitation can be achieved through various methods:
- Special contact lenses to correct corneal irregularities.
- Graft regularization treatments (TransPTK / topo- or wavefront-guided PRK) for contact lens intolerant patients to improve vision with glasses.
- Use of implantable contact lenses (ICL/IPCL) to reduce dependence on glasses.
Limitations:
- Grafts require a longer recovery, with sutures often remaining in place for several months.
- There is also a risk of graft rejection, requiring long-term monitoring.
Combinations of these different methods
Combining these different keratoconus treatment methods allows for a personalized approach based on:
- the severity of the disease
- the condition of the cornea
- The patient's visual needs.
The goal is to stabilize the cornea, improve vision, and prevent disease progression.
Treatment decisions are made in collaboration between the patient and the surgeon, taking into account the benefits and risks of each method.
Les différentes types de greffes
Découvrez les kératoplasties (= greffes de cornée)
Frequently asked questions
If you have any further questions, please do not hesitate to contact us!
How long does it take to recover after keratoconus surgery?
CXL (Cross-Linking): Recovery generally takes a few weeks. Vision gradually stabilizes over a period of 3 to 6 months.
Intracorneal Rings (ICRS/CAIRS): Initial recovery takes about a week, but full vision stabilization can take several months.
(Trans)PRK topo- or wavefront-guided + CXL: Recovery takes 1 to 2 weeks, but visual improvements continue for several months.
Corneal Transplant: Recovery is longer, potentially lasting several months to a year for complete healing and optimal visual clarity.
ICL/IPCL: Recovery is generally very quick, with improved vision without glasses noticeable just a few hours after the procedure. In cases of irregular cornea (e.g., keratoconus), a reduction in dependence on glasses is expected rather than complete independence.
What results can be expected from keratoconus surgery?
CXL (Cross-Linking): Primarily stabilizes the cornea and prevents disease progression. Some patients may also experience improved vision, but this is not guaranteed.
Intracorneal Rings (ICRS/CAIRS): Aim to improve the shape of the cornea and reduce visual distortions, but glasses or contact lenses are often still required.
PRK topo- or wavefront-guided: Generally improves vision quality and reduces irregular astigmatism, but does not always completely eliminate the need for optical correction.
Corneal Transplant: Can offer significant vision improvement, although glasses or contact lenses are usually still necessary after the procedure.
Implantable Contact Lenses (ICL/IPCL): Reduces reliance on optical aids for patients who have satisfactory vision with glasses.
How long do the results of cross-linking last for keratoconus treatment?
The results of cross-linking (CXL) are generally long-lasting, with most patients achieving stabilization of corneal shape and preventing keratoconus progression for many years. Studies suggest that, in the majority of cases, the effects are permanent, although regular follow-ups are essential to rule out and treat slow progression if necessary.
Is it possible to reduce dependence on glasses and contact lenses after keratoconus surgery?
If vision with glasses is satisfactory, it is possible to achieve a similar result through surgery using implantable contact lenses (ICL/IPCL).
To achieve satisfactory vision with glasses, it is sometimes necessary to regularize the cornea affected by keratoconus or the corneal graft using "resurfacing" laser (topography-guided transPTK/PRK) and/or intracorneal rings (ICRS/CAIRS) before proceeding with implantable contact lens surgery.
Linked surgical treatments
.avif)
.avif)

.avif)
Linked conditions
Book a consultation
Swiss Visio Montchoisi
1006 Lausanne, Switzerland